Diagnosis and treatment
of benign nail tumours
E. HANEKE
Dermatology Practice, Freiburg, Germany
Department of Dermatology, St Radboud University, Nijmegen,
The Netherlands
Department of Dermatology, Inselspital, Berne, Switzerland
SUMMARY:
The tip of the finger and toe form a functional unit with the nail organ. Tumours
of this particular region will therefore influence the shape, size and quality
of the nail and the entire distal phalanx and also exert profound effects on
the sensory function of the finger tip, the mobility of the finger and even
the hand or foot as a whole. Since the distal phalanx is made up of many different
tissue structures, a great variety of tumours may be observed, even those that
usually do not come to the attention of the dermatologist. On the other hand,
nail-specific tumours are rare, in contrast to neoplasms originating from the
hair follicle.
This article will give a brief overview of the most important tumours of the
distal phalanx and their treatment and prognosis.
Key words: Benign nail tumours, diagnosis, therapy, prognosis, melanonychia longitudinalis.
In the distal phalanx, almost
all skin tumours except those of the hair follicle may occur. In addition, the
bone of the terminal phalanx, cartilage, tendon sheath, blood and lymph vessels
as well as nerves may give rise to true tumours and reactive tumour-like lesions.
However, tumours comparable to those of the follicle but originating from the
nail matrix are very rare1.
Nail tumours are often difficult to diagnose, because the particular anatomical
conditions, specifically in subungual tumours, lead to a different growth pattern
and often to also different symptomatology. For instance, pain is a characteristic
symptom of fast-growing lesions, but may suggest a traumatic origin even though
this was not the cause. All changes hidden under the nail plate or proximal
nail fold should prompt a radiological examination. Xeroradiography is particularly
useful, as it avoids overexposure of the terminal phalanx, gives magnification
and often also allows evaluating the nail plate and soft tissues surrounding
the nail. A dental radiograph is an alternative, as this technique is specific
for the demonstration of small bony structures. Probing localises areas of most
intense pain, e.g. in subungual felon or glomus tumours, but also allows the
extent of an onycholysis to be evaluated. Transillumination, also termed diaphanoscopy,
gives information about potential cystic lesions and sometimes about a foreign
body, as it may give a sharply delimited shadow. Examination of the nail region
should be done with the fingers or toes in relaxed position, in extreme flexion
and extension, as well as with pressure of the digital tip on a hard surface,
as this allows evaluating the blood circulation. Dermatoscopy allows differentiating
melanin from haemoglobin and other pigments, it is almost as precise as capillary
microscopy and permits the visualisation of subungual foreign bodies and infestations
with scabies mites. Magnetic resonance imaging is useful for the diagnosis of
deep-seated lesions, particularly for subungual glomus tumours and submatrical
myxoid pseudocysts. High-resolution ultrasound may be used to measure nail plate
thickness.
The hand is one of the most cosmetically important regions, following the face
and the female breast. An intact and beautiful nail is of utmost importance
for the hand's look. However, the nail has more functions, such as those of
a mechanical tool and part of the sensory organ "fingertip". All surgical
interventions have to respect these particularities and require surgical skills,
in addition to a sterile operation theatre and fine instruments for atraumatic
surgery.
Benign and self-limited lesions, such as viral warts, must not be treated with
a technique leaving unsightly scars or a postoperative nail dystrophy. Recurrence
after removal of a benign tumour, such as a subungual keratoacanthoma, synovialoma
or recurrent infantile fibromatosis, should never be treated with amputation
of the digit.
Pre- and postoperative care has to be explained to the patient. Smoking is forbidden
until wound healing is complete. Antibiotic prophylaxis is considered beforehand,
particularly in case of ulcerated or infected lesions. An efficient tourniquet
is used to achieve a completely bloodless field whenever necessary. The tourniquet
is opened after 15-20 min to allow blood supply for approximately 3 min, and
then re-applied. Atraumatic surgery, fine instruments and a head magnifier lens
or surgical microscope are prerequisites for good nail surgery. Whenever possible,
the nail plate should remain in place or be replaced after surgery of benign
lesions, as this represents the best physiological dressing. It can be fixed
with mattress sutures and guarantees a much faster healing with fewer complications.
Benign tumours
and pseudotumours Viral warts
Subungual and
periungual warts are by far the most common tumour-like alterations of the nail
regions. They are mainly seen in children and adolescents. If warty lesions
develop in persons over 35 to 40 years and do not respond to wart treatment,
Bowen's disease should be considered for differential diagnosis. Warts are hard,
rough-surfaced, greyish, hyperkeratotic papules that often contain tiny black
dots corresponding to the histological phenomenon of thromboses in the tip of
the dilated capillaries. Whereas being round on the pulp of the digit the warts
are often oval or even crescentic and less hyperkeratotic on the proximal nail
fold or hyponychium. Deep fissures may cause pain. Subungual warts may even
erode the underlying bone2. Most commonly, human papillomavirus types 1, 2,
and 4 as well as 7 in butchers are found.
The differential diagnosis is important as in adults Bowen's disease may mimic
viral warts. Other diseases to be ruled out are subungual exostosis and other
tumours, tuberculosis cutis verrucosa etc.
Warts on the distal phalanx may be extremely recalcitrant. A surgical treatment
is however rarely indicated, since it not only will leave scars and sometimes
irreversible postoperative nail dystrophy, but its recurrence rate is as high
as that of conservative therapies. In situ hybridisation has shown that HPV
DNA may be found up to 15 mm around the wart.
We prefer an aggressive conservative approach with saturated monochloroacetic
acid (Acetokaustin in Germany). The solution is sparingly applied on the wart,
left to dry and then covered with 40 to 60% salicylic plaster (Guttaplast),
which is fixed with adhesive tape for a week. During this time, the patient
has to apply hot finger or footbaths twice daily, while leaving the salicylic
plaster on to stimulate the blood circulation; smoking should be interdicted.
After a week, the salicylic acid plaster is removed after another hot bath and
the necrotised keratin masses are gently removed with a curette. This procedure
is repeated until the warts are completely gone. This treatment is also applicable
in little children. Imiquimod after keratolysis and under occlusion is a new
alternative. Intralesional bleomycin injection may be very painful. The carbon
dioxide laser as well as curettage with a curette or ring scalpel require local
anaesthesia. In our hands, vascular lasers that are thought to dry out the warts
by coagulating its blood vessels do not work. Suggestive therapy is rarely effective
in this localisation. Wart treatment always takes much more time in smokers
than in non-smokers[3].
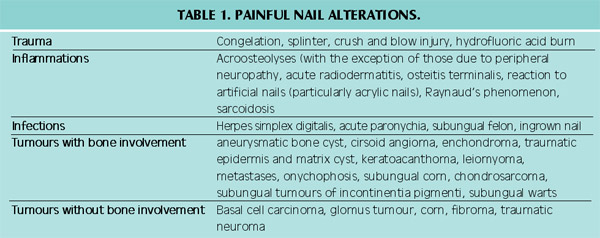
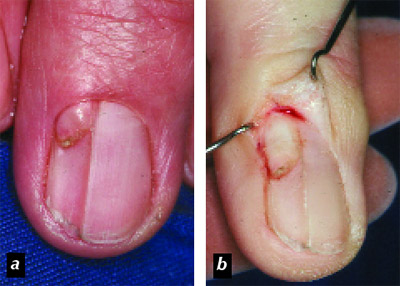
Figure 1. Epiungual fibrokeratoma
a. before surgery.
b. The origin of the lesion is visualised after opening the nail pocket.

Figure 2. Intraungual fibrokeratoma
partly covered by a nail plate lamella.
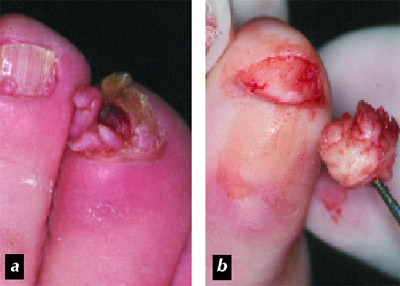
Figure 3. Koenen
tumours of tuberous sclerosis (Bourneville-Pringle disease): a. multiple ungual
fibromas of the 3rd toe, b. resection of the fibromas en bloc.
Figure 4. Eruptive
angioma (so-called pyogenic granuloma), a. before surgery, b. 10 days after
excision and closure of the primary defect with two flaps from the adjacent
skin of the proximal nail fold, c. 6 months after surgery, almost no scar is
visible and the nail plate is growing out completely normal; note the longitudinal
depression in the distal half of the nail plate from the pressure of the erauptive
angioma on the matrix.
Cysts
Of the many different cysts seen in the skin, only traumatic epidermal and postoperative
matrix cysts are seen in the distal phalanx.
Epidermal cysts usually present as slow growing space occupying process. Depending
on their location within the nail organ they may cause nail clubbing with increase
in nail size or bone erosion with an eventual fracture. Matrix cysts preferentially
develop after operations at the lateral matrix horn when matrix epithelium was
left in place. Most commonly, a nail spicule develops, more rarely a cyst containing
very hard keratin and the wall of which may histologically exhibit feature of
both epidermis and matrix epithelium. In elderly persons, metastases and slow-growing
osseous tumours have to be ruled out differential diagnostically. Complete extirpation
is the treatment of choice. Either a lateral L-shaped or a longitudinal nail
bed incision usually allows the lesion to be shelled out.
Onycholemmal
horn
This nail-specific lesion was observed in the lateral nail groove and adjacent
nail bed of elderly women. Clinically, an asymptomatic, markedly hyperkeratotic
lesion was seen. Histopathology showed a crateriform tumour filled with keratin
almost identical to the so-called trichilemmal horn. Clinically and histologically,
keratoacanthoma is the most important differential diagnosis.
Complete excision resulted in permanent cure[4].
Onychomatricoma
The onychomatricoma was described as an entity approximately 15 years ago. Its
clinical appearance is so characteristic that it can be diagnosed on clinical
grounds alone in most cases. There is a limited longitudinal thickening of the
nail with yellow discoloration and tiny splinter haemorrhages, and transverse
overcurvature. At the free nail margin, minute holes may be seen. After avulsion
of the nail, a villous tumour of the matrix is seen. The corresponding nail
plate shows holes into which the finger-like projections of the matrix tumours
fit. Longitudinal sections of the nail show canals in the nail substance that
are lined by matrix epithelium and extend distally to the free nail margin.
Total excision will lead to permanent cure, though there will be a postoperative
defect of nail growth depending on the size of the surgical specimen[1,5,6].
Subungual keratoacanthoma
The subungual localisation of keratoacanthoma is infrequent. In most cases,
it originates at the hyponychium, less frequently in the lateral groove, exceptionally
in the nail bed. Clinically, it is a rapidly growing tumour soon reaching the
underlying bone. Pain is characteristic. The clinical diagnosis may be difficult
when the nail plate covers the lesion. Cutting away the overlying nail will
reveal a tumour with a central horn plug. This is sometimes expressed during
surgery. Histopathology reveals a vertically oriented, keratin-filled tumour
that often reaches the bone and erodes it. Differential diagnostically, trauma,
foreign body, subungual warts and other tumours, particularly the non-tender
squamous cell carcinoma, have to be considered.
The excision has to reach down to the bone, maybe even include a lamella of
bone to avoid a recurrence. Mobilisation of the wound margins usually allows
the wound to be closed primarily. A small onycholytic area may be the only sequel[7].

Figure 5. Subungual glomus
tumour of the ring finger causing a red stripe in the nail bed.
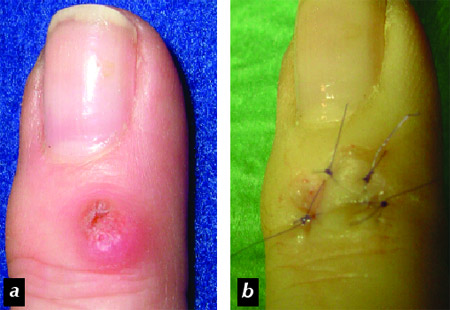
Figure 6. Recurrent myxoid
pseudocyst after removal with CO2 laser a. before re-operation, b. end of surgery
after raising a U-shaped flap, dissecting the degenrated myxoid connective tissue
and suturing the flap back into its original position.
Fibromas
of the nail organ
Fibromas are relatively frequently located on the distal phalanx. They may be
hereditary or acquired and differ in their histopathology[8,9]. Ungual fibromas
cause variable nail changes depending on their origin within the nail apparatus.
A deep canaliform depression is typical for those coming from the proximal matrix,
whereas nail bed fibromas cause a rim in the nail.
Ungual fibrokeratomas are the most frequent variety. Most of them come out from
under the proximal nail fold and cause a longitudinal depression. When their
origin is in the central matrix area, they run within the nail plate until the
overlying nail lamella breaks off showing the tip of the sausage-like tumour
(figure 1). Their distal end may be split into several free ends. The differential
diagnosis of early lesions is verruca vulgaris; long-standing lesions may resemble
a foreign body or a myxoid pseudocyst that penetrated through the proximal nail
fold's undersurface into the nail pocket.
The treatment of choice is its excision down to the bone in order to avoid a
recurrence. Fibrokeratomas lying on the nail plate (epiungual fibrokeratomas)
(figure 2) are excised with a Νο11 scalpel blade, which is held parallel to
the nail plate surface, thus permitting to incise around the base of the fibrokeratoma,
which is eventually severed from the bone with pointed curved scissors. The
same approach is used for intraungual fibrokeratomas; however, the overlying
nail plate lamella has to be removed before. The small defect does not require
a suture.
Subungual fibrokeratomas are excised from the distal matrix/nail bed accordingly.
A 6-0 PDS suture is recommended to close the small defect.
Koenen's tumours are a characteristic sign of tuberous sclerosis. From the age
of 10 to 12 years, they develop in approximately half of the patients. They
always occur in multitude and may destroy the entire nail organ if treatment
is delayed. Though most of them develop in the proximal and lateral grooves,
they may completely occupy the matrix and nail bed. They are excised at their
base without wound suture (figure 3). The cosmetic result depends on how much
healthy the nail tissue is[8-10].
Subungual filamentous
tumour
This rarely described lesion is certainly underdiagnosed. It usually presents
as a narrow whitish to yellowish, sometimes even brownish longitudinal stripe
in the nail that often causes nail splitting at its free margin. Clinical examination
reveals a small rim of keratin at the undersurface of the nail that may be pared
down painlessly. In case treatment is requested the nail plate is cut longitudinally
at both sides of the streak and elevated. The beginning of the lesion is seen
at the nail plate's underside in the distal lunula part and in the distal matrix
region as a tiny spike of tissue. This is removed by a saucer-shaped small excision,
which does not require a suture. However, recurrences are not uncommon[9].

Figure 7. Longitudinal melanonychia
due to a junctional naevus of the nail matrix.
Pyogenic
granuloma (teleangiectatium)
Granuloma pyogenicum is not a granuloma, but an eruptive angioma. When occurring
in the nail region, it is mainly seen on the nail fold or hyponychium. A pyogenic
granuloma penetrating the nail plate is commonly due to a perforating trauma.
The differential diagnosis of multiple pyogenic granulomas, coccal nail fold
angiomatosis, and granulation tissue is often very difficult, but other erosive
tumours including amelanotic melanoma and squamous cell carcinoma have to be
taken into consideration. Granulation tissue may also develop under treatment
with retinoids, some systemic antivirals, taxane type cytotoxic drugs[11-16].
Treatment of choice is its excision at the base and gentle electrocoagulation
of the central feeding artery. When located at the free margin of the proximal
nail fold, it should rather be excised with a wedge shaped nail fold excision.
The defect is closed after separation of the proximal nail fold from the underlying
nail plate, longitudinal incisions at both sides and suture of the central defect
(figure 4). This leaves to narrow secondary defects, which rapidly heal without
a visible scar[8]. Angiomas of the matrix and nail bed are removed by horizontal
excision and ligation of the feeder vessel. Electrocoagulation has to be kept
to a minimum in order to avoid scarring and postoperative nail dystrophy.
Glomus
tumour
The subungual glomus tumour is undoubtedly the best known of all nail tumours,
even though it is by far not the commonest. Its clinical symptomatology is so
characteristic that it is correctly diagnosed in most cases. However, patient
histories of decade-long suffering are known. The patients have increasing pain
in the distal phalanx exacerbating after minor shock or cold temperature and
radiating to the shoulder. Applying a finger tourniquet or a blood pressure
manchette pumped up to >200 mmHg makes the pain almost immediately disappear.
Clinically, a livid-red spot in the matrix or nail bed is seen, from which a
reddish stripe extends to the hyponychium (figure 5). The exact localisation
is found using a blunt probe: the point of most intense pain corresponds to
the glomus tumour. MRI is also useful to localise the lesion.
All painful lesions or those tender on touch or palpation have to be considered
in the differential diagnosis (table 1).
Glomus tumours in the lateral third of matrix or nail bed are extirpation via
a lateral L-shaped incision permitting the nail bed and matrix to be dissected
from the bone. The glomus tumour is seen as a greyish glassy round tumour, about
the size of a peppercorn or a pea[8,10,17]. Tumours in median position in the
matrix require avulsion of the overlying nail plate, either as a disc of nail
punched out with a 6mm diameter punch, or by incising the nail plate from its
lateral margin and detaching it from the nail bed in a trap-door manner. The
tumour is seen as a violet spot. The incision is performed over the tumour,
in transverse direction in the matrix, in longitudinal direction in the nail
bed. The soft grey nodule is meticulously dissected and shelled out. The defect
is sutured with 6-0 PDS stitches and the nail plate laid back. The pain disappears
within 2 to 3 days[10]. Wound healing is complete within 8 to 14 days, since
the replace nail plate considerably improves healing. Primary multiple or successive
glomus tumours may be the cause of persisting pain and may suggest recurrence[18].
Neurogenic
tumours
Neurogenic tumours of the distal digit are rare. Sometimes, a traumatic or amputation
neuroma develops after injury; however, there is no characteristic clinical
(table 1). Neurofibromas are very rare and almost always singular. Even in neurofibromatosis
von Recklinghausen with thousands of tumours on the rest of the body, ungual
neurofibromas are exceptional. Neurilemmomas, which are even less common than
neurofibromas, may be seen in the palmar side of the distal digit and cause
grotesque swelling. The treatment of choice is complete extirpation. The surgical
technique depends on the localisation within the nail apparatus or distal phalanx[7].
Synovialoma
Synovialomas sometimes develop in the distal phalanx. Dorsally located ones
form irregularly sized nodes that may resemble Heberden nodes. They may exert
pressure on the matrix, thus interfering with nail growth. They have to be excised
generously in order to avoid a recurrence. For precise dissection, a head magnifier
lens is required. Defect closure is achieved with a full-thickness skin graft.
Synovialomas in the pulp of the digit cause a considerable swelling of both
the pulp and the nail. The skin is opened with an L-shaped incision at the lateral
aspect of the distal phalanx and the yellowish-brown, corym-biform tumour is
completely extirpated. This is done by blunt dissection, as it has a fibrous
capsule in this localisation in contrast to synovialomas in dorsal position.
The histopathology shows a cellular tumour made up of histiocytes, fibroblast,
some foam cells, siderophages and characteristic osteoclast-like giant cells.
Minute calcifications seen on X-ray film are said to be a sign of malignancy.
Subungual
exostoses
Subungual exostoses are reactive lesions most commonly provoked by chronic repetitive
microtrauma. Their most common localisation is therefore the medio-dorsal aspect
of the distal hallux phalanx. Most patients are young adults, however they are
also seen in children and elderly persons. Bone fragments after fracture of
the distal phalanx may mimic an exostosis8,19. Whether or not subungual osteochondromas
represent a different entity is still under debate[20].
Clinically, most tumours are stone-hard nodes that elevate the nail plate. The
overlying epidermis is often thin and has lost its dermatoglyphic pattern, but
it may also be ulcerated. Confirmation of the diagnosis by radiograph is strongly
recommended, as it also allows the extent of the lesion to be determined. The
skin is incised and the bony lesion dissected. It is finally clipped off at
its base using a bone rongeur or a strong nail clipper. The wound is closed
with simple sutures.
The regrowing plate induces completely normal nail conditions. A final X-ray
is useful to control the extent of exostosis removal. When the exostosis is
under the nail the incision has to be adapted accordingly[10,21].
Myxoid
pseudocyst
This lesion is also called dorsal finger cyst. It is a relatively frequent degenerative
lesion occurring mainly in the second half of life. More than 90% are located
on the fingers, less than 10% on the toes. Women are more frequently affected.
An associated degenerative osteoarthritis of the distal interphalangeal joint,
often with Heberden nodes, is seen in most cases and probably of aetiological
significance. Clinically, a round, slightly dome-shaped, skin coloured to greyish-glassy,
soft to elastic tumour is seen in the proximal nail fold. Its pressure on the
matrix causes a longitudinal depression in the nail[10,22]. On the toes, it
is almost always a round transparent lesions bulging up, thus not causing a
canaliform depression in the nail. Primary subungual location is possible and
causes a rapidly developing limited overcurvature of the nail. The lunula takes
on a characteristic violaceous colour. Diaphanoscopy helps in making the diagnosis.
A variety of different treatments were proposed: multiple puncture and expression,
injection of steroid crystal suspension, of sclerosants, of hyaluronidase, cauterisation,
CO2-laser vaporisation[23], cryosurgery[24], simple excision and even amputation.
We have combined the methods of Kleinert and Newmeyer[25,26]: a minute amount
of sterile methylene blue (methyl thionine) is injected into the distal interphalangeal
joint through the volar crease just next to the flexor tendon; this allows the
true extent of the lesion to be seen. If the skin overlying the cystic lesion
is not too thin, a U-shaped or triangular flap is incised over and around the
lesion and raised. Since the lesion gains connection with the joint it will
be stained blue, as also the surrounding myxoid tissue. This is meticulously
dissected and the stalk to the joint is ligated using 6-0 PDS stitches.
Complete extirpation after previous demonstration of the lesion's extent with
methylene blue is superior to all other techniques described in the literature.
If the overlying skin is not too thin, a U-shaped incision around the distal
3/4 of the cyst is performed and the flap is cautiously dissected from distal
to proximal and the underlying degenerated tissue is removed. Any connection
with the distal interphalangeal joint -this is the case in more than 80%- will
be visible by the blue staining of the myxoid tissue and the pseudocyst; the
stalk to joint is seen as a dark blue spot. This is ligated with 6-0 PDS stitches.
The flap is laid back and sutured again. If the skin overlying the lesion is
very thin, it will be excised and a small rotation flap rose from the adjacent
skin to cover the defect. The resultant secondary defect rapidly heals by second
intention and the scar is soon almost invisible[22]. Primary subungual myxoid
pseudocysts are rare. They have to be removed via a transmatrical approach.
The proximal nail fold is separated from the underlying nail, incised at both
sides and reflected. The proximal part of the nail plate is detached from matrix
and cut transversely for about 2/3 to 3/4 of its width, this part is then reflected
like a trap door permitting access to the submatrical lesion. This is then dissected
and removed. The matrix incision is stitched with absorbable 6-0 PDS sutures.
A completely normal nail will regrow[8,22]. It is important to apply the postoperative
bandage in physiological flexion of the finger as joint stiffness is the most
common complication[27].
Melanocytic
alterations and brown nail pigmentations
Ungual melanoma is the most frequent and most serious malignant tumour of the
nail apparatus. About 65-75% of them are pigmented and usually give rise to
a longitudinal brown streak in the nail. This is why each acquired melanonychia
in fair-skinned adults has to be examined and considered potentially malignant
until otherwise confirmed[28-30]. Since there is no clear-cut clinical difference
between nail pigmentation due to a melanoma or to a benign melanocytic lesion,
their differentiation with any possible means is of utmost importance.
Brown
and black pigments
Brown and black nail pigmentation is usually due to melanin, microbial pigments,
subungual or deeply intraungual blood, or exogenous substances, such as silver
nitrate. Often the nature of the pigment can be suggested on clinical grounds
and histology and/or biochemistry can confirm this assumption. For histopathology
or histochemistry, the free margin of the nail plate is useful when the pigmentation
involves it. Subungual keratosis is examined when it contains pigment. Superficial
pigmentations may be diagnosed from a tangentially excised piece or a punched-out
disc of nail.
Blood is the commonest cause or dark nail colorations. A single, almost always
very painful trauma (see table 1), for instance due to a hammer blow or crush
in a door, is remembered by the patient and is no diagnostic challenge. Just
over the haematoma, a small leukonychotic area is often seen as a sign of the
injury to the fibrous keratin structure of the nail plate. The matrix and/or
nail bed tissue disrupts from the power of the trauma and blood gets under the
nail plate. Any haematoma occupying more than half of the nail area is suspicious
of a fracture of the terminal phalanx and should prompt an X-ray. Any bone dislocation
has to be corrected to avoid later nail dystrophy. The pain after an acute trauma
rapidly disappears when a small hole is drilled over the haematoma to allow
it to be evacuated. Diagnostic problems may however arise in subungual haematomas
of the great toe, particularly in lateral position, since their development
is usually overlooked because the chronic microtrauma was not noticed. Hiking,
skiing and other sports are the most common cause. An important differential
diagnostic sign is that these haematomas do not reach the free margin of the
nail and have an oval shape in contrast to melanocyte-derived longitudinal melanonychia.
The dried blood under the nail usually grows out, but in rare cases it may be
non-migratory. A small hole may then be punched into the nail and some of the
pigment scraped out. This is collected in a small test tube, some drops of water
are added, mixed, and with a haemostix such as is used to search for blood in
urine, the true nature of the pigment can be revealed. The subungual blood pigment
remains Prussian-blue negative, as it is not degraded to haemosiderin; this
test is however extremely sensitive and will react to the smallest amount of
blood that may come from injuring the nail bed during collection of the material.
In addition, all bleeding tumours are also positive[28].
Microbial pigments are chemically different. Various pathogenic and harmless
fungi produce melanin as resistance and virulence factors, e.g. in onychomycosis
nigricans[31]. The fungal melanin is soluble and not particulate, it therefore
remains negative with the argentaffin reaction of Fontana-Masson. In a pale
haematoxylin-eosin or PAS stain, this melanin appears as a diffuse yellowish
colour of the nail. Heavily pigmented fungi may stand out by their dark colour.
In most cases, both nail plate and subungual keratin can be clipped and used
for histopathological and mycological examinations. Clinically, a dark spike
is seen with its broad base at the distal margin of the nail plate, which rarely
reaches to the matrix. Several black stripes or an extensive staining may occur
in one nail. Trichophyton rubrum var. nigricans is the most common cause of
fungal melanin. The commonest bacterial pathogens causing dark nail coloration
are Pseudomonas aeruginosa, Klebsiella and Proteus spp. A greenish colour is
in favour of Pseudomonas. Very often, the pigmentation is at the lateral margin
of the nail plate, sometimes emerging from under the nail fold. In contrast
to human melanin, it may be scraped off the surface, but soon recurs.
Exogenous pigment stains the surface and can often be scraped off or removed
by tangential sectioning of the nail. It grows out with a proximal border parallel
to the free margin of the proximal nail fold. Manganese dioxide, which develops
from potassium permanganate used as a disinfectant, stains the nail and the
surrounding skin. It can be removed with ascorbic acid wipes that reduce the
dioxide to a colourless compound. Heavy smokers not only have a stained side
of the nail, but also of the adjacent skin. Etching of granulations, for instance
due to ingrowing nails, or of oozing tumours with silver nitrate stains the
tissue jet-black including the nail plate. Black silver nitrate granules are
seen in the upper layers of the nail plate in histological sections. The silver
stain grows out with the nail[32].
Human melanin is finely granular, intracellular in the onychocytes and is argentaffin[10,
33]. Single pycnotic melanocytes in the nail plate are a sign of subungual melanoma
that exhibits a pagetoid melanoma cell spread in the matrix epithelium leading
to intraungual melanoma cells[34]. The localisation of the melanin in the nail
plate gives a hint at its origin: pigment in the lower nail plate stems from
the distal matrix, that in the medial layers from the medial matrix, and that
in the dorsal nail plate from the proximal matrix. Pigment in the entire thickness
of the nail means that the whole length of the matrix is involved. The colour
may reach from light brown to black, but in Caucasians different shades of brown
are the commonest. The band forms when a focus of pigment-producing melanocytes
consistently gives more melanin to the onychocytes than they can degrade normally
so that they still contain pigment granules during the process of onychisation.
However, the demonstration of melanin in the nail alone does not allow a diagnosis
to be made. A biopsy from the origin of the stripe, the matrix is necessary;
a nail bed biopsy is too distal and will not give the information required[33].
Nail
pigmentation in dark-skinned persons
Melanin-induced brown to black streaks in the nail are rare in fair-skinned
persons, but rather the rule in dark-skinned people. Since dark-skinned individuals
develop melanomas much less frequently than light-skinned ones, however, acral
lentiginous and ungual melanomas are as frequent as in fair-skinned, the differential
diagnosis may be very difficult. Brown pigmentation of many finger and toenails
are in favour of a benign process. When a single streak stands out by a jet-black
coloration a malignant melanoma should be suspected and a histopathological
examination of a matrix biopsy is mandatory[35].
Longitudinal
melanonychia
There are no clinical criteria to reliably differentiate a benign or malignant
melanonychia. Some observations are in favour of a malignant process:
- The pigmentation developed at age >30 years
- The acquired stripe is wider than 5mm
- The streak develops a periungual pigmentation: Hutchinson's melanotic whitlow
- The pigment stripe darkens or becomes wider proximally indicating growth of
the pigment cell nidus in the matrix
- A nail dystrophy develops in the pigmented area
- An erosive or bleeding nodule develops.
Melanonychia striata longitudinalis usually reflects a circumscribed increase
in the number of melanocytes, a Lentigo or a junctional melanocytic naevus;
however, even at that age subungual melanoma may occur[36-38]. We therefore
advocate a histological examination to rule out malignant melanoma. Since most
dermatologists are not experienced in taking a nail matrix biopsy, this is often
performed too late.
Biopsy
techniques
There are different possibilities to take a biopsy for the diagnosis of a longitudinal
melanonychia[28-30].
1. Pigment band in the lateral third of the nail: lateral longitudinal nail
biopsy
Starting at the distal dorsal crease of the distal interphalangeal joint, a
straight incision is carried out down to bone through the proximal nail fold,
matrix, nail bed, nail plate and hyponychium medial from the stripe in the nail
plate. A second incision is performed parallel to the first one but along the
lateral nail plate margin and in the lateral nail groove. This slender long
tissue block is dissected from the bone using pointed curved iris scissors.
Care has to be taken not to leave remnants of the lateral matrix horn, behind
from which a recurrence might develop. The defect is closed with back-stitches
that elevate the lateral nail fold, thus improving the cosmetic aspect after
the biopsy[39, 40]. This biopsy leaves a narrower, but otherwise normal appearing
nail. The tissue block gives an excellent histological overview of the entire
pathological process. However, experience from the side of the pathology laboratory
is required both in handling of the specimen and of the histopathological interpretation.
2. Localisation of a pigmented
band less than 3mm wide in the median part of the nail: punch biopsy of the
matrix
Since a matrix defect of maximally 3mm diameter will only leave a narrow red
band after wound healing, a punch of 3mm may be used for very narrow melanonychia.
The beginning of the stripe, which is usually hidden under the proximal nail
fold, is crucial to biopsy. The punch is run down to bone and the tissue cylinder
sectioned at its base with curved pointed scissors. Since the melanocyte focus
in the matrix is often larger than anticipated, clinically marginal recurrences
are not uncommon. We therefore recommend to remove the nail plate portion overlying
the melanocyte nidus and to completely excise it[28,29].
3. Localisation of a pigmented
band less than 3mm wide in the median part of the nail: fusiform excision
A pigmented band in the central portion of the nail that is wider than 3mm does
no longer permit a punch excision. The proximal nail wall is incised at both
sides and reflected. The overlying nail plate is detached and also reflected
to one side. The beginning of the stripe is now visible. This allows the entire
melanocytic lesion to be observed and excised in a transverse fusiform manner
with a small safety margin of about 1mm. The matrix is gently mobilised and
sutured with 6-0 absorbable stitches; care has to be taken not to tie the sutures
too tight, in order to avoid their cutting through the fragile matrix tissue.
The degree of postoperative nail dystrophy depends on the necessary extent of
the matrix excision.
4. Localisation of a wide
pigmented band in the median or lateral nail portion: horizontal excision of
the pigment cell lesion
Our own data and recent publications have shown that longitudinal melanonychia
in young persons is most commonly due to a lentigo or junctional naevus in the
matrix[37,38,41] (figure 7). Melanocytes are then not found in the dermis. We
have therefore developed a biopsy technique that does not leave a cicatricial
nail dystrophy. The proximal nail fold is reflected. The proximal third of the
nail plate is sectioned transversely, detached from the matrix and opened, allowing
the pigment cell focus to be visualised. A very superficial incision is carried
around the lesion with a small safety margin. The lesion is horizontally excised
in a manner as if taking a free matrix graft. The nail plate, to which the superficial
third of the matrix epithelium adheres, is laid back and fixed with two mattress
sutures. The proximal nail fold is sutured back. Wound healing was uneventful
and without any postoperative nail dystrophy in more than 30 cases operated
with this technique[42,43]. The thin slice of tissue is spread out on a little
piece of filter paper and then immersed into the fixative. Histological examination
is possible without delay. In case of a benign lesion, no further treatment
is necessary. In case of a malignant melanoma, a generous re-excision will follow.
Conclusion
Considering the anatomy and histology of nail tumours and respecting the rules
of atraumatic sterile surgery, excellent functional and cosmetic results can
usually be achieved if the patient comes early enough to surgery10.
Mailing
address:
Prof. Dr Eckart Haneke
Schlippehof 5
79110 Freiburg im Breisgau
Deutschland
Τel.: 0049 178 5927764
Mob.: 0049 761 8978368
E-mail: haneke@gmx.net
References
1. Haneke E. Intraoperative
differential diagnosis of onychomatricoma, Koenen's tumours, and hyperplastic
Bowen's disease. 7th Cong Eur Acad Dermatol Venereol - Eur Nail Soc, Nice. J
Eur Acad Dermatol Venereol 1998; 13:Suppl (S119).
2. Baran R, Haneke E. Tumours of the nail apparatus and adjacent tissues. In:
Baran R, Dawber RPR, eds. Diseases of the Nails and their Management. Blackwell,
Oxford 1994, p. 417-497.
3. Haneke E. Differentialdiagnose und Therapie von Schwielen, Huhneraugen und
Plantarwarzen. Z Hautkr 1982; 57:263-272.
4. Haneke E. Onycholemmal Horn. Dermatologica 1983; 167:155-158.
5. Haneke E, Franken J. Onychomatricoma. Dermatol Surg 1995; 21:984-987.
6. Kint A, Baran R, Geerts ML. The onychomatricoma: an electron microscopic
study. J Cut Pathol 1997; 24:183-188.
7. Haneke E, Mainusch O, Hilker O. Subunguale Tumoren: Keratoakanthom, Neurofibrom,
Nagelbett-Melanom. Z Dermatol 1998; 184:86-102.
8. Haneke E. Cirurgia dermatologica de la region ungueal. Monografias de Dermatologia.
1991; 4:408-423.
9. Haneke E. The spectrum of ungual fibromas. [Abstract], Dermatology 2000,
Singapore 1998.
10. Haneke E, Baran R, Bureau H. Chirurgie der Nagelregion. Z Hautkr 1982; 57:1107-1116.
11. Blumental G. Paronychia and pyogenic granuloma-like lesions with isotretinoin.
J Am Acad Dermatol 1984; 10:677-678.
12. Baran R. Retinoids and the nails. J Dermatol Treat 1990; 1:151-154.
13. Bouscarat F, Bouchard C, Bachour D. Paronychia and pyogenic granuloma of
the great toes in patients treated with indinavir. N Engl J Med 1998; 338:1776-1777.
14. Pierson JC, Owens NM. Pyogenic granuloma-like lesions associated with topical
retinoid therapy. J Am Acad Dermatol 2001; 45:967-968.
15. Baran R. Pyogenic granuloma-like lesions associated with topical retinoid
therapy. J Am Acad Dermatol 2002; 47:970.
16. Sass JO, Jakob-Solder B, Heitger A, Tzimas G, Sarcletti M. Paronychia with
pyogenic granuloma in a child treated with indinavir: the retinoid-mediated
side effect theory revisited. Dermatology 2000; 200:40-42.
17. Ekin A, Ozkan M, Kabaklioglu T. Subungual glomus tumours: A different approach
to diagnosis and treatment. J Hand Surg 1997; 22B:228-229.
18. Ali Noor M, Masbah O. Synchronous glomus tumors in a distal digit: A case
report. J Hand Surg 1997; 22A:508-510.
19. Stieler W, Reinel D, Janner M, Haneke E. Ungewohnliche Lokalisation einer
subungualen Exostose. Akt Dermatol 1989; 15:32-34.
20. de Palma L, Gigante A, Specchia N. Subungual exostosis of the foot. Foot
Ankle Int 1996; 17:758-763.
21. de Berker D, Langtry J. Treatment of subungual exostoses by elective day
case surgery. Br J Dermatol 1999; 140:915-918.
22. Haneke E. Operative Therapie der myxoiden Pseudozyste. In: Haneke E, ed.
Fortschritte der operativen Dermatologie. Bd 4: Gegenwartiger Stand der operativen
Dermatologie. Springer-Verlag Berlin, Heidelberg 1988, p. 221-227.
23. Street M, Roenigk R. Recalcitrant periungual verrucae : The role of carbon
dioxide laser vaporization. J Am Acad Dermatol 1990; 23:115-120.
24. Dawber RPR, Sonnex T, Leonard J, Ralfs I. Myxoid cysts of the finger: treatment
by liquid nitrogen spray cryosurgery. Clin Exp Dermatol; 8:153.
25. Kleinert HE, Kutz JE, Fishman JH, McCraw LH. Etiology and treatment of the
so-called mucous cyst of the finger. J Bone Jt Surg 1972; 54A:1455-1458.
26. Newmeyer WL, Kilgore ES, Graham WP. Mucous cysts: the dorsal interphalangeal
joint ganglion. Plast Reconstr Surg 1974; 53:313-315.
27. Fritz RG, Stern PJ, Dickey M. Complications following mucous cyst excision.
J Hand Surg 1997; 22B:222-225.
28. Baran R, Haneke E. Diagnostik und Therapie der streifenformigen Nagelpigmentierung.
Hautarzt 1984; 35:359-365.
29. Baran R, Haneke E. Management of longitudinal melanonychia. 17th World Congr
Dermatol 1987; Vol Abstr II:568.
30. Baran R, Kechijian P. Longitudinal melanonychia (melanonychia striata):
diagnosis and management. J Am Acad Dermatol 1989; 21:1165-1175.
31. Perrin C, Baran R. Longitudinal melanonychia caused by Trichophyton rubrum.
Histochemical and ultrastructural study of two cases. J Am Acad Dermatol 1994;
31:311-316.
32. Haneke E. Silver nitrate staining of the nail. Collegium Dermato-Pathol,
Turin 1998.
33. Haneke E. Clinical judgment. A lesson derived from a subungual melanoma.
Dermatopathol Pract Concept 2000; 6:73-76.
34. Kerl H, Trau H, Ackerman AB. Differentiation of melanocytic nevi from malignant
melanomas in palms, soles, and nail beds solely by signs in the cornified layer
of the epidermis. Am J Dermatopathol 1984; 6(Suppl 1):159-161.
35. Kopf AW, Waldo E. Melanonychia striata. Australas J Dermatol 1980; 21:59-70.
36. Haneke E. Laugier-Hunziker-Baran-Syndrom. Hautarzt 1991; 42:512-515.
37. Leaute-Labreze C, Bioulac-Sage P, Taieb A. Longitudinal melanonychia in
children. A study of eight cases. Arch Dermatol 1996; 132:167-169.
38. Goettmann-Bonvallot S, Andre J, Belaich S. Longitudinal melanonychia in
children: A clinical and histo-pathological study of 40 cases. J Am Acad Dermatol
1999; 41:17-22.
39. Haneke E. Behandlung einiger Nagelfehlbildungen. In: Wolff HH, Schmeller
W (Herausg) Fehlbildungen - Navi - Melanome. Fortschritte der operativen Dermatologie
1985; 2:71-77, Springer, Berlin - Heidelberg - New York.
40. Haneke E. Reconstruction of the lateral nail fold after lateral longitudinal
nail biopsy. In: Robins P, ed. Surgical Gems in Dermatology. Journal Publ Group,
New York NY, 1988: 91-93.
41. Tosti A, Baran R, Piraccini BM, Cameli N, Fanti PA. Nail matrix nevi: a
clinical and histopathological study of twenty-two patients. J Am Acad Dermatol
1996; 34:765-767.
42. Haneke E. Operative Therapie akraler und subungualer Melanome. In: Rompel
R, Petres J (Hrsg). Operative und onkologische Dermatologie. Fortschritte der
operativen und onkologischen Dermatologie 1999; 15:210-214, Springer, Berlin.
43. Haneke E. Tangential matrix excision for longitudinal melanonychia (2006,
in preparation).